Circulation

Human circulatory system
Table of Contents
Blood
Blood is composed of a liquid, plasma, and blood cells such as erythrocytes (red blood cells,) leukocytes (white blood cells), and platelets (cell fragments). Hematocrit is the percentage of blood volume occupied by the erythrocytes.
Plasma
Consists of a number of inorganic and organic substances: nutrients, metabolic wastes, and hormones dissolved in water. It also contains the following:
- bilirubin (the product of hemoglobin breakdown)
- albumin (synthesized by the liver)
- globulin
- fibrinogen – functioning in clotting.
The plasma from which all proteins have been removed is called serum.
Blood cells
(1) Erythrocytes
The erythrocytes carry oxygen and carbon dioxide by binding them with iron in hemoglobin. They have a high surface-to-volume ratio. The plasma membrane of erythrocytes has surface proteins and polysaccharides that confer blood group. Reticulocytes, produced in the soft interior of bones, called bone marrow, lose their cell organelles and enter the circulation as erythrocytes. At the end of their lives, the erythrocytes are degraded in the liver and the spleen. Iron, folic acid, and vitamin B12 are important constituents.
Iron: the homeostatic control of iron balance resides in the intestinal epithelium. Iron is stored in the liver as ferritin. Iron released from the degraded erythrocytes is carried to the bone marrow by plasma protein transferrin, and incorporated into new erythrocytes.
Regulation of Erythrocyte Production: erythrocyte production is stimulated by a hormone called erythropoietin, secreted mainly by kidneys.
Anemia: A decrease in the ability of blood to carry oxygen may be due to:
- A decrease in the total number of erythrocytes
- A lower concentration of hemoglobin per erythrocyte
- A combination of both
Sickle cell anemia results in the abnormal shape of hemoglobin due to a genetic mutation. Polycythemia is an excess of erythrocytes that results in a lower flow of blood in capillaries.
(2) Leukocytes
There are 3 types of polymorphonuclear granulocytes (characterized by having multilobed nuclei and granules): (1) eosinophils, (2) basophils, and (3) neutrophils (most abundant), monocytes and lymphocytes. All leukocytes are produced in the bone marrow. These cells participate in immune defense.
Platelets
Platelets are colorless cell fragments that enter the circulation when cytoplasmic portions of bone marrow cells called megakaryocytes are pinched off. Their primary function is in the blood clotting process.
Regulation of Blood Cell Production
In children, the marrow of most bones produces blood cells whereas in adults only the bones of the upper body produce blood cells. All blood cells descend from a single population of bone marrow cells called pluripotent hematopoietic stem cells. These cells can divide into (1) pluripotent stem cells, (2) lymphoid stem cells that give rise to lymphocytes, or (3) myeloid stem cells that give rise to all other types of blood cells. Division and differentiation of these cells are regulated by protein hormones and paracrine agents, collectively called hematopoietic growth factors (HGFs).
Design of Cardiovascular System
Rapid blood flow in one direction is called bulk flow. This is produced by pumping action of the heart. The high branching of blood vessels ensures the proximity of all cells to some capillaries. Nutrients and metabolic end products move between capillary blood and interstitial fluid by diffusion.
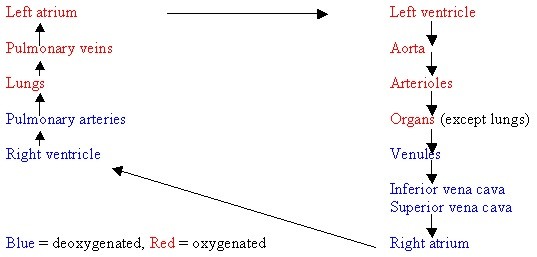
The heart is longitudinally divided into 2 halves: left and right, and each half contains two chambers: the upper atrium and the lower ventricle. The atrium on each side is connected to the ventricle on that side but there is no connection between the two atria or the two ventricles. Blood is pumped out of the heart through one set of vessels and returns to the heart via another set. Vessels carrying blood away from the heart are called arteries while those carrying blood toward heart are called veins.
Pulmonary circulation (through lungs for oxygenation) Systemic circulation (to extremities and back)
Pressure, Flow, and Resistance
Blood flows from a region of high to a region of low pressure and rate of blood flow (F) is given
F=Δp/R
where:
Δp is the difference in pressure between two points
R is resistance to flow
R, in turn, is determined by the viscosity of blood and length & radius of blood vessels.
Under most physiological conditions, changing the radius of blood vessels controls the flow of blood. (i.e. vasoconstriction, vasodilation)
Heart Anatomy
The heart is a muscle enclosed in a sac called the pericardium. The walls of the heart are composed of cardiac muscle cells called myocardium. A thin layer of cells called endothelial cells lines the inner surface. Located between the atrium and ventricle on each side are the atrioventricular (AV) valves. The right AV valve is called the tricuspid valve and the left AV valve is called the mitral valve. The valve at the opening of the right ventricle into the pulmonary artery is called a pulmonary valve. The valve where the left ventricle enters the aorta is called the aortic valve and these two valves are also called semilunar valves. These valves will only allow blood to flow in one direction and their opening and closing is a passive process resulting from pressure differences across the valves.
Cardiac muscle
Cardiac muscle cells are striated. The desmosomes and the gap junctions at the structures called intercalated disks join adjacent cells. Some cells do not function in contraction but they do form the conducting system that initiates the heartbeat and spreads it throughout the heart. These muscle cells are obviously vital and they are innervated with a rich supply of sympathetic fibers that release norepinephrine and parasympathetic fibers that release acetylcholine. Blood supply to cardiac muscle cells is supplied and drained by the coronary arteries and the coronary veins, respectively. Blood that is pumped through the chambers does not exchange substances with the cells of the heart muscle.
Heartbeat coordination
The sequence of excitation. A group of nerve cells called the sinoatrial (SA) node in the right atrium depolarizes first. The discharge rate of the SA node determines the heart rate. Depolarization quickly spreads to the left atrium and the two atria contract simultaneously. The action potential then spreads to ventricles after a small delay through the atrioventricular (AV) node that is located at the base of the right atrium. The delay in the action potential allows atrial contraction to be completed before the ventricle contracts. The potential then spreads to the ventricles via the bundle of His (atrioventricular bundle) and the Purkinje fibers and both ventricles contract simultaneously. The capacity of the SA node for spontaneous, rhythmical self-excitation is a result of gradual depolarization (the pacemaker potential) of the cells. Depolarization, in turn, occurs when Na+ channels open once again during the repolarization phase of the previous potential.
Electrocardiogram. Electrical events in the heart can be indirectly recorded at the surface of the skin from the currents generated in the extracellular fluids. An EKG (ECG) recording should consist of 3 deflections: (1) P wave – the atrial depolarization, (2) QRS complex – the ventricular depolarization, and (3) T wave – the ventricular repolarization. The long refractory period of heart muscle cells limits the re-excitation of cardiac nerve cells, thus inhibiting tetanus.
Mechanical events of the cardiac cycle
The cardiac cycle is divided into two phases:
- Systole: the phase of ventricular contraction and blood ejection. During the first part of the systole phase, the ventricles contract while all valves are still closed and therefore no blood is ejected. This period is called the isovolumetric ventricular contraction. The volume of blood ejected from each ventricle is called the stroke volume (SV). The amount of blood remaining after ejection is called the end-systolic volume (ESV).
- Diastole: the phase when the ventricles relax and blood fills into the chambers. During the first part of the diastole, the ventricles relax while all valves are still closed. This period is called isovolumetric ventricular relaxation. The amount of blood in the ventricle at the end of diastole is called end-diastolic volume (EDV).
SV = EDV – ESV
Cardiac output
To find the volume of blood pumped by each ventricle per minute:
CO = HR x SV Cardiac output equals heart rate multiplied by stroke volume.
Control of Heart Rate. SA node is innervated by the autonomic nervous system. Activity in parasympathetic nerves releases Ach, which close Na+ channels and decreases the slope of pacemaker potential, causing the heart rate to decrease. Activity in sympathetic nerves releases norepinephrine, which then opens Na+ channels and increases the slope of pacemaker potential, causing the heart rate to increase.
Control of Stroke Volume. A more forceful contraction of the ventricle can cause a greater emptying of the ventricle, thus increasing stroke volume.
EDV & SV: Frank-Starling Mechanism. The greater the EDV means the greater stretching of the ventricular muscles. This also means producing a more forceful contraction. Cardiac muscle is normally not at its optimal length (lo). Thus, additional stretching increases the force of contraction. In sum, as the end-systolic volume decreases, the overall stroke volume increases.
Sympathetic nerves release norepinephrine, which can increase myocardial contractility by increasing calcium infusion.
Vascular System
Arteries
The arteries are large, elastic tubes lined at the interior by the endothelial cells. Arterial walls have connective tissue and smooth muscles. During systole, contraction of ventricles ejects blood into arteries, distending the arterial walls. During diastole, the walls recoil passively and more blood is driven out. There is always some blood in the arteries to keep them semi-inflated. Maximum arterial pressure reached during systole is called systolic pressure (SP), and minimum arterial pressure reached during diastole is called diastolic pressure (DPI). The difference between SP and DP is called pulse pressure (PP). The average pressure driving blood into tissues is called mean arterial pressure (MAP).
Arterioles
The arterioles contain smooth muscles that can relax to increase vessel radius (vasodilation) or contract to decrease vessel radius (vasoconstriction). It controls blood flow through an organ. This can be calculated with this formula:
Forgan = MAP / Resistanceorgan
Local controls. Local controls are mechanisms independent of hormones and nerves. Hyperemia occurs when the blood flow in an organ increases by arteriolar dilation in response to an increase in metabolic activity that causes local changes such as a decrease in O2 or an increase in CO2 and H+.
Extrinsic controls. Sympathetic nerves provide a rich supply of impulses to the arterioles. Upon activation, the arterioles release norepinephrine to cause vasoconstriction. Hormones such as vasopressin (from posterior pituitary) and angiotensin II (from the liver) constrict arterioles.
Capillaries
Capillaries permeate every tissue in the body to provide front line access to cells in order to exchange nutrients and metabolic end products.
Anatomy of the Capillary Network. A capillary is a thin-walled tube of endothelial cells one layer thick resting on a basement membrane without any surrounding muscle or elastic tissue. The endothelial cells are separated from each other by narrow, water-filled spaces called intercellular clefts.
The velocity of Capillary Blood Flow. Blood velocity decreases as blood passes through the huge cross-sectional area of a capillary.
Diffusion and Exchange across Capillary Wall. There are three basic mechanisms by which substances move across capillary walls to enter or leave the interstitial fluid:
- Diffusion is the only important means by which the net movement of nutrients, oxygen, and metabolic end products can occur. Intercellular clefts allow the passage of polar molecules. Brain capillaries, however, are tight with no intercellular clefts. Liver capillaries are leaky with large clefts for the movement of substances. The transcapillary diffusion gradient is set up by the utilization or production of a substance.
- Vesicle transport allows for the passage of molecules via endo- and exocytosis.
- Bulk flow enables protein-free plasma to move from capillaries to the interstitial fluid due to hydrostatic pressure. This is opposed by an osmotic force, resulting from differences in protein concentration that tends to move interstitial fluid into the capillaries. Bulk flow also serves to function in distributing extracellular fluid.
The net filtration pressure (NFP) can be calculated by:
NFP = Pc – PIF – πP + πIF
Where:
Pc = capillary hydrostatic pressure (favoring fluid movement out of capillary)
PIF = interstitial fluid hydrostatic pressure (favoring fluid movement into capillary)
πP = the osmotic force due to plasma protein concentration (favoring fluid movement into capillary)
πIF = the osmotic force due to interstitial fluid protein concentration (favoring fluid movement out of capillary)
These four factors are called Starling forces.
Veins
Veins are thin-walled, low resistance vessels that carry blood from the tissues to the heart.
Determinants of Venous Pressure. Total blood volume is an important determinant of venous pressure. At any given time, most of the blood is in the veins. The walls of the veins are more elastic and thus can accommodate large volumes of blood with a relatively small increase in pressure. The walls contain smooth muscle innervated by sympathetic neurons that release norepinephrine. This constricts vessels that increase pressure and drive more blood. During the contraction of the skeletal muscle, the veins in the muscle are compressed. This reduces the vein diameter resulting in increased pressure. This is called skeletal muscle pump. When the diaphragm descends during inspiration, there is increased pressure in intraabdominal veins and a decreased pressure in intrathoracic veins, increasing venous pressure. This is called the respiratory pump. Venous valves prevent the backflow of blood in veins.
Lymphatic System
The lymphatic system is a network of small organs (lymph nodes) and tubes (lymphatic vessels) through which lymph flows. Lymph is a fluid derived from the interstitial fluid. Lymphatic capillaries are composed of a single layer of endothelial cells resting on a basement membrane. Their water channels are permeable to all interstitial fluid components, including protein. Interstitial fluid enters these capillaries by bulk flow and the fluid flows through lymph nodes and ends in two lymphatic ducts that drain into subclavian veins in the lower neck. Lymphatic vessels carry interstitial fluid back to the cardiovascular system and compensate for net filtration out of blood capillaries. Additionally, the lymphatic system provides a pathway by which fat absorbed in the gastrointestinal tract reaches the blood. Infections causing blockage of the lymphatic system leads to an accumulation of interstitial fluid, called edema.
Mechanism of Lymph Flow
Lymph is propelled by the rhythmical contractions of smooth muscle lining the walls of lymphatic vessels. The contractions are triggered by the stretching of the walls when lymph enters the system. Lymphatic vessels have valves to produce a one-way flow. The vessels are innervated by sympathetic neurons and are also influenced by the skeletal muscle pump and the respiratory pump.
Regulation of Systemic Arterial Pressure
Mean arterial pressure is determined by cardiac output and total peripheral resistance (TPR). TPR is the sum of resistance to flow offered by all systemic blood vessels.
MAP = CO x TPR
Arteriolar resistance is the main determinant of TPR. Any deviation in MAP elicits homeostatic reflexes so that CO or TPR is changed to minimize the deviation.
Baroreceptor reflexes
- Arterial baroreceptors. These are the short-term regulators of MAP. Pressure receptors are present in the carotid sinus at the neck, the aortic arch (aortic arch baroreceptors), pulmonary vessels, wall of the heart, and large systemic veins. Afferent neurons, the firing rate of which is positively correlated to MAP, from these receptors travel to the brainstem.
- Medullary cardiovascular center. This is the primary integrating center for baroreceptor reflexes in the brainstem medulla oblongata. When arterial baroreceptors decrease their discharge as a result of less MAP, sympathetic outflow increases, increasing heart rate, ventricular contractility, and vasoconstriction. It also elicits an increased secretion of Angiotensin II and vasopressin, which constrict arterioles.
Blood volume
Long term regulation of MAP is dependent upon blood volume. An increase in MAP decreases blood volume by increasing the excretion of salt and water by kidneys, consequently bringing down MAP.
Hemorrhage and Other Causes of Hypotension
Hypotension is low blood pressure due to low blood volume. SV, CO, MAP decrease as a direct result of hemorrhage and arterial baroreceptor reflexes work to restore them to normal. HR and TPR increase as reflex responses due to increases in sympathetic outflow. Interstitial fluid is moved into the vascular system due to reduced capillary pressure. In the long term, fluid ingestion and kidney excretion are altered and erythropoiesis is stimulated to replace blood volume. Loss of large quantities of cell-free extracellular fluid through sweating, vomiting, diarrhea, etc. also invoke similar symptoms and responses. Hypotension can cause fainting. Hypotension can be an indicator of the insufficiencies of the autonomic nervous system.
Shock
Tissue or organ damage due to reduced blood flow is called shock.
- Hypovolemic shock is caused by a decrease in blood volume due to hemorrhage or loss of fluid
- Low-resistance shock is due to a decrease in TPR due to excessive release of vasodilators, as in allergy and infection
- Cardiogenic shock due to a decrease in CO (cardiac output), as in a heart attack.
Upright Posture
There is a decrease in the effective circulating blood volume during the transition from a horizontal to a vertical position. In a horizontal position, all blood vessels are at the same level and almost all pressure is due to cardiac output. In a vertical position, there is an additional pressure at every point, equal to the weight of the blood column from the heart to that point. This results in distension of blood vessels due to the pooling of blood and increased capillary filtration in lower parts of the body. The effect of gravity can be offset by the contraction of skeletal muscles in the legs.
Exercise
As CO increases, there is increased blood flow to muscles and skin (to dissipate heat). CO is increased by a large increase in HR – caused by increased activity in the SA node, and a small increase in SV caused by increased ventricular contractility mediated by sympathetic activity. There is also an increase in EDV and the Frank-Starling mechanism comes into play. Venous return is promoted by: (1) increased activity in skeletal muscle pump and (2) increased activity in respiratory pump inspiration (due to increased depth and frequency of inspiration). Control mechanisms for these cardiovascular changes involve feedforward regulation, active hyperemia, resetting of arterial baroreceptors.
Maximal Oxygen Consumption and Training
Oxygen consumption increases in proportion to the magnitude of exercise until a point maximal oxygen consumption (VO2max). After VO2max is reached, any further increase in work can be only briefly sustained by anaerobic metabolism. VO2max is limited by: (1) CO, (2) the ability of the respiratory system to deliver oxygen to the blood, and (3) the ability of muscles to use oxygen. Normally, VO2max is determined by cardiac output.
Hypertension
Increased arterial pressure is generally due to an increased TPR resulting from the reduced arteriolar radius. Renal hypertension results from increased secretion of renin, which generates angiotensin II – a vasoconstrictor. Hypertension results in an increase in muscle mass of the left ventricle (left ventricular hypertrophy) since it has to pump against increased arterial pressure. This could decrease contractility leading to heart failure.
Heart Failure
In heart failure, the heart fails to pump an adequate CO. In diastolic dysfunction, the wall of the ventricle has reduced compliance and has a reduced ability to fill adequately resulting in reduced EDV and therefore a reduced SV. Systolic dysfunction results from myocardial damage and results in a decrease in cardiac contractility and a lower SV. Adaptive reflexes to counter the reduced CO results in (1) fluid retention and can cause edema – one in the lung can impair gas exchange, and (2) increased TPR makes it harder for the heart to pump.
Coronary Artery Disease and Heart Attacks
In coronary artery disease, changes in the coronary arteries cause insufficient blood flow (ischemia) to heart, resulting in damage to the myocardium (myocardial infarction or heart attack). Chest pains associated with this are called angina pectoris. Ventricular fibrillation triggers abnormal impulse conduction by damaged myocardial cells resulting in uncoordinated ventricular contractions. The major cause of coronary artery disease is atherosclerosis – a thickening of the arterial wall due to (1) abnormal smooth muscle, (2) cholesterol deposits, or (3) dense layers of connective tissue. The thickened wall reduces blood flow and also releases vasoconstrictors. Atherosclerosis of a cerebral artery can lead to localized brain damage – a stroke or reversible neurologic deficits called transient ischemic attacks (TIAs). Coronary thrombosis is the total occlusion of a blood vessel by a blood clot.
Hemostasis – Prevention of Blood Loss
Hemostasis is the stoppage of bleeding from small vessels. Venous bleeding leads to less rapid blood loss because veins have lower blood pressure. Accumulation of blood in tissue as a result of bleeding is called a hematoma. When a blood vessel is severed, it constricts and the opposite endothelial surfaces of the vessel stick together to slow the outflow. It is followed by other processes including clotting.
Formation of a platelet plug
Injury to a vessel exposes the underlying connective tissue collagen, and platelets bind to the collagen via an intermediary called von Willebrand factor (vWF) – a plasma protein secreted by endothelial cells and platelets. Binding of platelets to collagen triggers the release of secretions from platelets that change the shape and surface proteins of platelets (platelet activation), causing them to stick together (platelet aggregation) and creating a platelet plug. The platelet plug acts as a primary sealer. The plug does not expand away from the damaged endothelium because intact endothelium synthesizes and releases prostacyclin (prostaglandin 12, PGI2) that inhibits platelet aggregation.
Blood coagulation: clot formation
Blood is transformed into a solid gel, called a clot or thrombus, that consists mainly of the protein fibrin. It supports and reinforces the platelet plug. Plasma protein prothrombin is converted to the enzyme thrombin, which then catalyzes the formation of fibrin from fibrinogen. Platelets are essential to clot formation since they provide the surface on which many of the reactions occur. Vitamin K is required as a precursor to produce prothrombin and other clotting factors. Plasma calcium is also required for this process.
Anticlotting systems
The fibrinolytic (thrombolytic) system removes the clot after the vessel is repaired. Plasminogen activators activate a plasma proenzyme, plasminogen to the enzyme plasmin that digests fibrin to dissolve the clot.
Common anticlotting drugs
Aspirin, Heparin, Streptokinase

Fun activity: Label the heart, a worksheet from Science Learning Hub
You will also like...

Sensory Systems
A sensory system is a part of the nervous system consisting of sensory receptors that receive stimuli from the internal ..
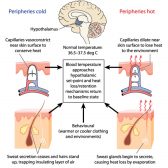
Temperature Regulation in Animals
This tutorial elucidates body temperature regulation. Know the details here to learn how the body sets the body temperat..
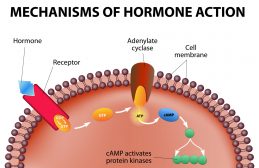
Homeostatic Mechanisms and Cellular Communication
Homeostasis is the relatively stable conditions of the internal environment that result from compensatory regulatory res..

Adaptation Tutorial
Adaptation, in biology and ecology, refers to the process or trait through which organisms or the populations in a habit..

Indicator Species and Endangered Species
Certain species are capable of expressing characteristics indicative of the state of the ecosystem they occupy. They are..

Effect of Chemicals on Growth & Development in Organisms
Plants and animals need elements, such as nitrogen, phosphorus, potassium, and magnesium for proper growth and developme..